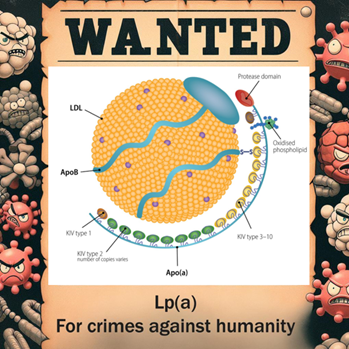
It’s been quite a week for news about the Felons of the Lipid Neighborhood, (which you can read more about in Chapter 6 of THIS BOOK) and since we all know the news can be pretty depressing, I’ll get back to writing about my daughter’s stories and baking sourdough soon enough! But this new study from the UK Biobank about Lp(a), risk of VTE (venous blood clots), menopause, and hormone replacement therapy should provide you with some “food for thought” in the meantime.
When a clot forms, plasminogen can be converted to plasmin to dissolve the clot, because when clots don’t dissolve, you’re having a pretty bad day. Lp(a) bears a significant resemblance to plasminogen and since the LPA gene is on chromosome 6 right next to the PLG (plasminogen) gene, it’s popular to state that Lp(a) is just “preventing plasminogen from clot busting.” Well, Lp(a) does seem to interfere with normal thrombolysis (clot busting), but not EXACTLY for that reason…lipids are rarely that simple. And despite the strong associations between Lp(a) and ASCVD, aortic stenosis, peripheral artery disease, and other pathologic states, we haven’t consistently observed that same association between elevated Lp(a) and VTE in genetic studies or prospective trials.
Well, there is a LOT to unpack from this study, so I’ll give you the key takeaways so that we can all get back to bread-making!
Key Takeaways
–For those with Lp(a) levels >125 nmol/L (the preferred particle measurement of how many Lp(a) “Felons” are in your Lipid Neighborhood), premenopausal women had a 32% increased VTE risk. This was in a group of over 55,000 women, and this didn’t seem to have anything to do with use of oral contraceptives (OCPs). This same risk of VTE was NOT found in the 129,000 postmenopausal women as a whole (or the 189,000 men…that’s the last time we mention the guys), BUT…
-For those POSTMENOPAUSAL women with Lp(a) levels >125 nmol/L who were on HORMONE REPLACEMENT THERAPY, there was a 48% increased VTE risk. There were 9,289 women in this group.
-For both premenopausal and postmenopausal groups, the risk of VTE in those with high Lp(a) was magnified at higher levels of serum estradiol (the primary circulating estrogen). Each doubling of estradiol levels strengthened the association between Lp(a) and VTE by 46%. This is interesting, as estrogen suppresses the basal production of Lp(a), so Lp(a) levels can rise, in some cases quite significantly, during the menopausal transition, which is thought to increase risk of cardiovascular disease. However, post-menopausal HRT, particularly oral estrogen, decreases Lp(a) levels modestly, but is there a trade-off when it comes to VTE risk? This study did not differentiate between transdermal and oral estrogen or progesterone/progestin usage or duration of HRT, further muddying the already cloudy waters! And there are other factors that can contribute to increased VTE risk as well.
In summary:
This is an interesting hypothesis-generating study. Perhaps there are hormonal influences that could lead the Lp(a) Felons of the Lipid Neighborhood to commit venous crimes rather than arterial infractions in females. Maybe the signal was due to other factors and we need to better assess the type of hormonal therapy administered to these populations. Regardless, studies of this nature should encourage all clinicians to individualize care and take a nuanced approach to patient management.
And now, back to baking sourdough!